
Mediscare: The Surprising Truth
Republicans are being portrayed as Medicare Grinches, but ObamaCare already has seniors' health care slated for draconian cuts.
By THOMAS R. SAVING
AND JOHN C. GOODMAN
WSJ.com
The Obama administration has repeatedly claimed
that the health-reform bill it passed last year
improved Medicare's finances. Although you'd never
know it from the current state of the Medicare
debate—with the Republicans being portrayed as the
Medicare Grinches—the claim is true only because
ObamaCare explicitly commits to cutting health-care
spending for the elderly and the disabled in future
years.
Yet almost no one familiar with the numbers thinks that the planned brute-force cuts in Medicare spending are politically feasible. Last August, the Office of the Medicare Actuary predicted that Medicare will be paying doctors less than what Medicaid pays by the end of this decade and, by then, one in seven hospitals will have to leave the Medicare system.
But suppose the law is implemented just as it's
written. In that case, according to the Medicare
Trustees, Medicare's long-term unfunded liability
fell by $53 trillion on the day ObamaCare was
signed.
But at what cost to the elderly? Consider people
reaching the age of 65 this year. Under the new law,
the average amount spent on these enrollees over the
remainder of their lives will fall by about $36,000
at today's prices. That sum of money is equivalent
to about three years of benefits. For 55-year-olds,
the spending decrease is about $62,000—or the
equivalent of six years of benefits. For
45-year-olds, the loss is more than $105,000, or
nine years of benefits.
In terms of the sheer dollars involved, the law's
reduction in future Medicare payments is the
equivalent of raising the eligibility age for
Medicare to age 68 for today's 65-year-olds, to age
71 for 55-year-olds and to age 74 for 45-year-olds.
But rather than keep the system as is and raise the
age of eligibility, the reform law instead tries to
achieve equivalent savings by paying less to the
providers of care.
What does this mean in terms of access to health care? No one knows for sure, but it almost certainly means that seniors will have difficulty finding doctors who will see them and hospitals who will admit them. Once admitted, they will enjoy fewer amenities such as private rooms and probably a lower quality of care as well.

Seniors attend a "Medicare Monday" seminar in Centennial, Co., to learn how federal health care reform will affect Medicare and their personal health insurance plans.
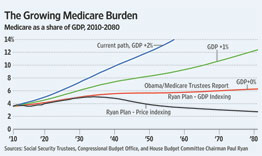
Are there better ways of solving the problem? The
graph nearby shows three proposals, including the
new law, and compares them to the current system.
For the past 40 years, real Medicare spending per
capita has been growing about two percentage points
faster than real gross domestic product (GDP) per
capita. Since real GDP per capita grows at just
about 2%, that means Medicare is growing at twice
the rate of our economy—and is clearly
unsustainable. If nothing is done, we'll see a
doubling of the Medicare tax burden in less than 20
years.
There are currently an array of proposals to slow
Medicare spending to a rate of GDP growth plus 1%.
These include a proposal by President Obama's debt
commission, chaired by Bill Clinton's former chief
of staff, Erskine Bowles, and former Sen. Alan
Simpson; one by former Clinton budget director Alice
Rivlin and Rep. Paul Ryan (R., Wis.); and another by
former Sen. Pete Domenici and Ms. Rivlin. Unlike the
Medicare Trustees, the Congressional Budget Office
(CBO) also scores ObamaCare at GDP plus 1%.
Of greater political interest is the House
Republican budget proposal, sponsored by Mr. Ryan.
This proposal largely matches the new law's Medicare
cuts for the next 10 years and then provides new
enrollees with a sum of money to apply to private
insurance (premium support). Even though the CBO
assumed premium support would increase with consumer
prices (price indexing), the resolution that House
Republicans actually voted for contains no specific
escalation formula. A natural alternative is letting
premium support payments grow at the annual rate of
increase in per-capita GDP (GDP indexing).
In light of the heated rhetoric of recent days,
it is worth noting that for everyone over the age of
55, there is no difference between the amount of
money the House Republicans voted to spend on
Medicare and the amount that the Democrats who
support the health-reform law voted to spend. Even
for younger people, the amounts are virtually
identical with GDP indexing.
The law's spending path depends on making
providers pay for all the future Medicare
shortfalls. But since no one can force health-care
providers to show up for work, short of a
health-care provider draft this reform ultimately
cannot succeed. The House Republican path, on the
other hand, would make a sum of money available to
each senior to choose among competing private
plans—much the way Medicare Advantage provides
insurance today for about one out of every four
Medicare beneficiaries.
That's a good starting point. But we believe that
a truly successful overhaul of Medicare will require
at least three additional elements.
First, there must be general system reform. You
cannot credibly hold senior health-care spending way
below everyone else's spending, nor can we make
taxpayers pay for all the future elderly's health
care. We must create a reform that reduces the rate
of growth of health-care costs for everyone—young
and old.
The best reform proposal for the non-elderly,
interestingly, is a health plan Mr. Ryan has
cosponsored with Sen. Tom Coburn (R., Okla.). It
would give all Americans the same tax relief for
health insurance and encourage market forces to
constrain costs.
Second, if federal spending is to be contained,
young people need to be able to save in tax-free
accounts during their working years in order to
replace the dollars they will not be getting from
Medicare.
Finally, providers need to be able to repackage and reprice their services under Medicare in ways that lower costs and improve quality. Anyone who saves Medicare a dollar should be able to keep 25 cents (or some other significant amount). Once that happens, private-sector innovations will spring up overnight.
Mr. Saving is director of the Private Enterprise Research Center at Texas A&M University and served two terms as a public trustee of the Social Security and Medicare Trust Funds. Mr. Goodman is president and CEO of the National Center for Policy Analysis.